
A tongue-tied baby has a short, thick, or tight lingual frenulum under the tongue, and that can limit how the tongue moves. For some babies, it causes no trouble at all, but for others it can lead to feeding problems and, later, speech concerns.
If you’ve noticed a poor latch, long feeds, clicking sounds, or nipple pain, you’re not overreacting. These signs can point to tongue-tie, though they can also have other causes, so a clear look at symptoms matters. For many families, getting the facts early makes feeding feel less stressful and more manageable, especially when paired with healthy breastfeeding support.
Keep reading to see what tongue-tie looks like, what causes it, how it’s diagnosed, and when treatment helps.
How tongue-tie affects a baby’s mouth and feeding
Tongue-tie can change how a baby uses the mouth during feeding. The issue is usually about movement, not looks, and that matters because feeding depends on the tongue working like a small, flexible pump and seal.
Some babies manage just fine with a mild tie. Others struggle right away because the tongue cannot move well enough to latch, draw milk, and keep a steady suck. The difference comes down to function, which is why a full feeding assessment matters more than a quick glance.

What the frenulum does under the tongue
The lingual frenulum is the small strip of tissue under the tongue that connects it to the floor of the mouth. In a baby with normal movement, that tissue stays flexible and lets the tongue lift, stretch forward, cup around the breast or bottle nipple, and move side to side.
Those motions matter during feeding. A baby needs to lift the tongue to create suction, extend it to take a deep latch, and cup it to hold milk in the mouth. Side-to-side movement also helps the tongue gather milk and keep the latch steady.
When the frenulum is short or tight, the tongue may look pinned down or less mobile. A tied tongue can still move some, but not always enough to work well during feeding. For a clear overview of how tongue-tie is described in infants, the NHS tongue-tie guide gives a simple explanation.
A tongue-tie does not have to look severe to cause trouble. If the tongue cannot move well, feeding can be affected.
Why limited tongue movement can cause feeding trouble

Feeding works best when the tongue can lift and seal the breast or bottle nipple in place. If the tongue stays low or tight, the baby may not latch deeply, and that can lead to a shallow latch, weak suction, and less milk transfer.
You may notice a baby popping off the breast, making clicking sounds, or feeding for a long time without seeming satisfied. Air swallowing can happen too, which often means more gas and more fussiness after feeds. The AAP clinical report on ankyloglossia also stresses that feeding problems are judged by function, not appearance alone.
Common signs of limited tongue movement during feeding include:
- Shallow latch that does not stay secure
- Clicking or loss of suction during nursing
- Popping off the breast or bottle often
- Long, tiring feeds with little milk transfer
- Extra air swallowing, which can lead to gas or discomfort
Severity can range from mild to more obvious, and that range matters. Some babies with a visible tongue-tie feed well because the tongue still moves enough. Others struggle because even a small restriction blocks the motions needed for an effective latch and good milk flow. In short, tongue mobility is what counts, because feeding depends on how the tongue works, not just how it looks.
If feeding is hard, the next step is usually a careful look at latch, milk transfer, and positioning, along with support such as smoother newborn feeding routines.
Signs your baby might be tongue-tied
Tongue-tie often shows up at feeding time first. Some babies have obvious signs, while others look fine at a glance and still struggle with milk flow, latch, or comfort.
The clues usually fall into two groups, baby signs and parent signs. Both matter, because a baby can be working hard even when the tie is not easy to see.
Feeding signs parents often notice first

Feeding trouble is usually the biggest clue. A baby with tongue-tie may have a hard time getting a deep latch, then keep unlatching and relatching as if the nipple keeps slipping away.
You may also notice slow feeds, noisy sucking, or a clicking sound. These signs often point to weak suction and poor milk transfer. Milk can dribble from the mouth, and feeds may drag on without much payoff.
Watch the diaper count too. Fewer wet or dirty diapers can mean baby is not taking in enough milk, especially in the early weeks. Gentle concerns about poor weight gain can also come up when feeding is tiring and milk transfer is low.
Common feeding clues include:
- trouble latching at the breast or bottle
- frequent unlatching during feeds
- slow, tiring feeds
- dribbling milk from the mouth
- clicking, smacking, or noisy feeding
- fewer wet or dirty diapers than expected
If these patterns sound familiar, a feeding check can help. The Johns Hopkins tongue-tie guide explains how tongue movement can affect latch and milk transfer.
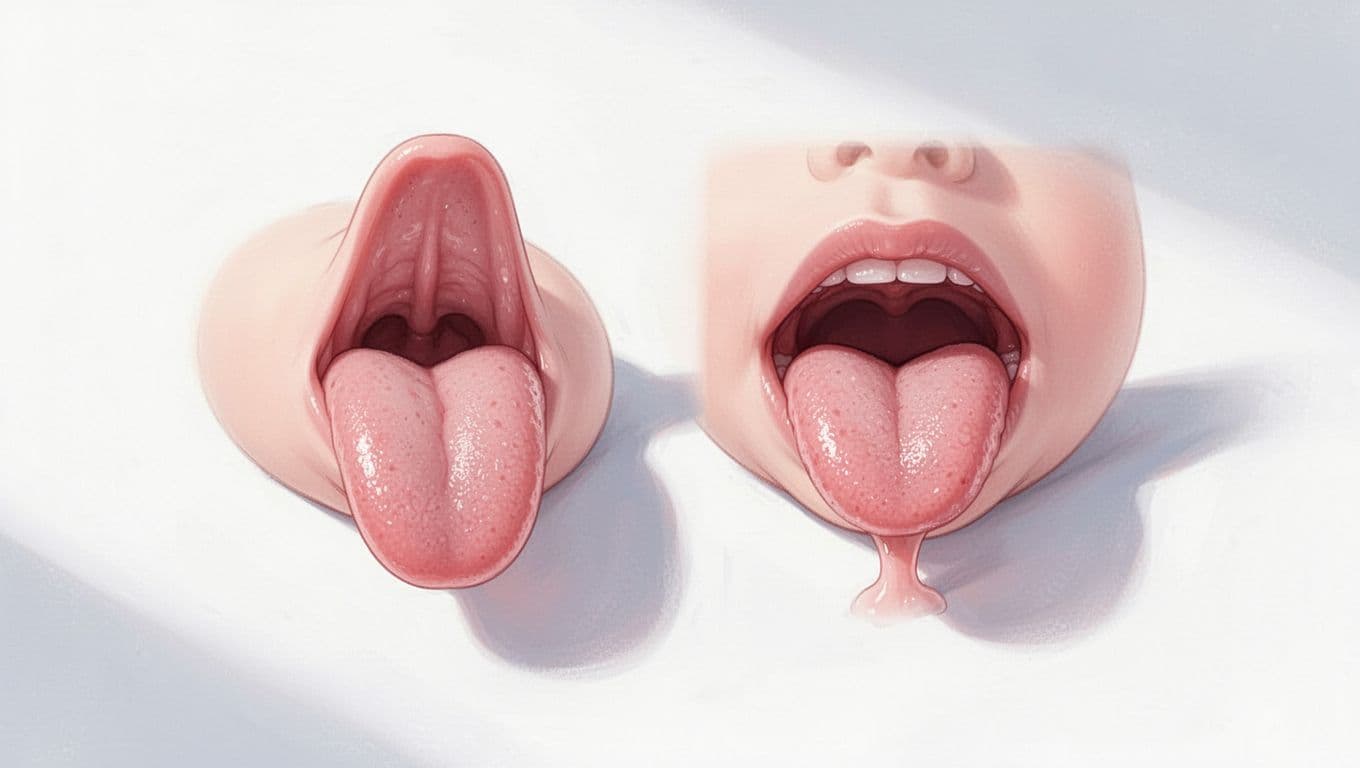
What a tongue-tied tongue can look like

A tongue-tied tongue can have a heart-shaped or notched tip when it lifts. Some babies cannot stick the tongue out past the lower lip, and others cannot lift it well toward the roof of the mouth.
You might also notice that the tongue looks pulled down in the middle or seems less flexible than expected. These visual clues can be helpful, but they do not confirm a problem by themselves. A baby can have a visible tie and feed well, or have a less obvious tie and still struggle.
Appearance alone does not tell the full story. Tongue movement and feeding function matter more than a quick look.
That is why doctors and lactation consultants look at both the mouth and the feeding session. The tongue may look short or tight, yet the real question is whether it can move enough to work well.
Symptoms nursing parents may feel

For nursing parents, pain is often the first red flag. A tongue-tied baby may latch in a way that causes nipple pain, cracking, pinching, or damaged skin, especially when the latch stays shallow.
Some parents also deal with repeated mastitis, plugged ducts, or worries about low milk supply. If baby cannot remove milk well, the breast may not drain fully, and that can make feeds feel frustrating on both sides.
Still, pain alone does not prove tongue-tie. Nipple soreness can also come from a poor latch for other reasons, engorgement, thrush, or positioning issues. If feeding hurts, it makes sense to get help early instead of guessing.
A few parent signs to pay attention to:
- sharp pain at latch-on
- nipples that look pinched or misshapen after feeds
- cracked or bleeding nipples
- repeated breast infections or plugged ducts
- frustration or dread before feeds
If low milk supply is also a concern, these breastfeeding supply tips may help while you sort out the cause. And if your baby also seems hard to settle, newborn calming routines can make feeding days feel a little less chaotic.
What causes tongue-tie and how common it is
Tongue-tie starts before birth, and in many babies, it seems to happen when the tissue under the tongue does not thin out or separate fully. That leaves the frenulum shorter or tighter than usual, which can limit how the tongue moves after birth.
Most cases are present at birth, and many are mild. Some never cause a problem, while others show up fast during feeding.
Why it happens before birth
During early development, the tongue and the tissue under it change shape as the baby grows. In a typical pregnancy, that thin band becomes flexible enough to let the tongue move freely.
With tongue-tie, that process does not finish in the usual way. The tissue stays a little too tight, too short, or too close to the tongue tip. As a result, the tongue may not lift, extend, or cup the way it should.

This happens before a baby is born, so parents do not cause it. It is a development issue, not something related to feeding choices after delivery. The Mayo Clinic explanation of tongue-tie gives a clear overview of how the frenulum stays attached in tongue-tie.
Is tongue-tie inherited?
Family patterns do show up, so genetics may play a role. If a parent, sibling, or close relative had tongue-tie, the chance can be a little higher.
Still, many babies with tongue-tie have no known family history. That makes the cause feel less predictable, because there is no single pattern that explains every case.
Tongue-tie often runs in families, but it can also appear without warning in a baby with no known history.
Tongue-tie is usually not linked to a major health problem on its own. Most babies with it do not have other medical concerns. In some rare cases, it can appear with certain genetic syndromes, but that is not the norm. A review in NCBI’s medical literature on ankyloglossia notes that most cases happen without other birth defects.
How common tongue-tie is
Tongue-tie is fairly common in newborns, but the exact rate depends on how it’s diagnosed. Some studies find lower numbers, while others find more, especially when clinicians use a structured exam instead of a quick visual check.
A good rule of thumb is that it affects a small but not rare share of babies, and it shows up more often in newborns than older children. The reported rate changes because different providers look for different signs, and mild cases are easy to miss.
A recent meta-analysis in Pediatric Research found an overall prevalence near 8% in infants under 1 year, while other reviews report a broader range. Boys are diagnosed more often than girls, and most babies with tongue-tie are otherwise healthy.
A few reasons the numbers vary:
- some clinicians diagnose by appearance alone
- others focus on how well the tongue moves
- feeding problems are not always the same from one baby to another
- mild cases may never get counted
So, the main takeaway is simple: tongue-tie is common enough that many parents hear about it, but not every baby with a tight frenulum needs treatment. The real question is whether it affects feeding, comfort, or growth.
How doctors check for tongue-tie
Doctors check tongue-tie with a hands-on exam and a feeding history. They look at how the tongue moves, how the frenulum sits under the tongue, and whether the baby is having real feeding trouble.
That matters because a tongue-tie diagnosis is never based on looks alone. A baby can have a visible frenulum and still feed well, so the exam has to focus on function.
What providers look for during an exam

During the exam, a doctor, pediatrician, lactation consultant, or ENT specialist usually starts with a close look under the tongue. They may gently lift the tongue, check whether it can move side to side, and see how far it can extend or rise toward the roof of the mouth.
They also watch a feeding session when they can. That gives a much clearer picture than a quick look in the office, because the tongue has to work during a real latch. A baby who seems fine at rest may still struggle once feeding starts.
The exam is usually simple and does not need special testing. In many cases, the provider uses a physical exam, a feeding observation, and a few basic questions about latch, nipple pain, milk transfer, and weight gain. The Mayo Clinic tongue-tie diagnosis guide explains that this is often enough to make the call.
What providers often check includes:
- how well the tongue lifts
- how far the tongue moves out and side to side
- whether the frenulum looks tight or restrictive
- how baby latches and stays on the breast or bottle
- signs of poor milk transfer, like long feeds or low diaper output
Sometimes a provider may use a scoring tool, but that tool does not replace the exam. The key question stays the same: is the tongue restriction getting in the way of feeding?
A good diagnosis starts with function. If the baby feeds well, a visible frenulum may not need treatment.
Why function matters more than appearance
A visible frenulum can look dramatic, yet still cause no problem at all. Some babies have a short or noticeable band under the tongue and feed normally from day one.
That is why treatment decisions should come from the baby’s feeding pattern, weight gain, and family concerns. If nursing hurts, feeds take too long, or weight gain is slow, those signs matter more than a photo of the tongue shape.
Doctors also look at the bigger picture. Was the latch shallow from the start? Is the baby swallowing well? Is the parent dealing with cracked nipples or repeated pain? These details help separate a true tongue-tie problem from other feeding issues, like positioning or milk supply concerns.
The best approach is practical and calm. A baby with feeding trouble may need further evaluation, while a baby with a visible tie but normal feeding may just need watching. A recent systematic review on infant tongue structure and function found that both structure and feeding impact need to be considered together.
If the exam shows clear restriction and real feeding problems, the provider may discuss next steps. If not, they may recommend support, follow-up, and a closer look before deciding on treatment.
What happens if tongue-tie causes problems
When tongue-tie causes problems, the main issue is usually feeding first. A baby may work harder for less milk, and that can affect comfort, growth, and the whole feeding routine.
In some babies, the tie stays mild and never becomes a real concern. In others, the tight frenulum gets in the way of latch, suction, and tongue movement, so the problems show up fast and keep building.
Breastfeeding challenges that can build up quickly
A poor latch can turn every feed into a struggle. If the tongue cannot lift and extend well, the baby may not transfer milk efficiently, so feeds last longer and end with a still-hungry baby.
That pattern can lead to ongoing hunger, slow weight gain, and feeding fatigue. Babies may tire out before they get enough milk, then want to feed again soon after. Over time, that cycle can wear down both baby and parent.
For the nursing parent, the pain can be just as hard. A shallow latch often causes sore nipples, cracking, or a pinched feeling that makes each feed stressful. When pain keeps showing up, some parents start dreading feeds, and that stress alone can make breastfeeding feel unmanageable.

If milk transfer stays low, early weaning becomes more likely. Some families can work through it with lactation support, but others reach a point where feeding hurts too much or takes too long to continue. The AAP clinical report on ankyloglossia notes that feeding problems need to be tied to function, not just how the tongue looks.
Possible speech and eating concerns later on

Later on, tongue-tie can sometimes affect speech sounds that need precise tongue movement, such as t, d, s, z, l, or th. It may also make certain oral tasks harder, like licking food, clearing food from the teeth, or moving food around the mouth.
That said, speech outcomes vary a lot. Many children with tongue-tie speak clearly and eat normally without treatment. Others never develop speech problems at all, even if the frenulum still looks tight.
A few later signs may stand out:
- trouble licking lips or an ice cream cone
- food left behind in the mouth
- difficulty moving food side to side
- speech that stays hard to understand after the usual age range
Tongue-tie matters most when it affects function. A visible tie alone does not mean a child will have speech trouble.
If you’re unsure whether a tongue-tie is causing real problems, a feeding or speech check can help sort out what’s normal variation and what needs attention. For a broader look at early mouth and language development, newborn play and language activities can also support healthy oral growth through simple daily interaction.
Treatment options, from lactation help to frenotomy
Treatment depends on function, not just the diagnosis. If a tongue-tie is mild and feeding is going well, many babies need only support and time. When feeding stays hard, though, the goal is to improve latch, reduce pain, and help baby take milk more easily.
The usual path starts with conservative care. If that does not solve the problem, frenotomy may be discussed, especially when tongue-tie is clearly affecting feeding or comfort.
When feeding support may be enough

For many families, the first step is feeding support. Small changes in position can make a big difference. A deeper latch, better head support, or a shift in angle can help the tongue work more effectively.
A lactation consultant can watch a full feed and spot problems you may miss at home. They can help with latch, positioning, milk transfer, and pumping plans when needed. That extra support often helps mild tongue-tie cases improve without a procedure.
Helpful changes may include:
- trying different nursing positions
- working on a deeper latch
- supporting baby’s head and body alignment
- checking bottle flow if bottle-feeding
- watching diaper counts and weight gain
If feeding improves with support, a procedure may not be needed at all.
This approach matters because some babies simply need time and better technique. When the tie is mild, the tongue may still move well enough once the latch is fixed. A feeding plan that works is the win, even if the frenulum still looks short.
What frenotomy is and how it works
Frenotomy is a quick procedure that snips the tight frenulum under the tongue. Families may hear it called a tongue-tie release or frenotomy, but the idea is the same, freeing the tongue so it can move more normally.
In many cases, it’s done in the office and takes only a few minutes. Babies usually recover fast, and feeding can often resume right away. The AAP notes that frenotomy is reasonable when breastfeeding problems continue after lactation support has been tried.
The procedure is simple, but it still deserves a careful decision. It’s usually considered when tongue-tie is causing clear feeding trouble, such as poor latch, low milk transfer, or ongoing nipple pain. The latest AAP clinical report on ankyloglossia supports trying nonsurgical help first, then moving to frenotomy only when symptoms persist.
Recovery is often quick, with little downtime. Still, follow-up matters because the real question is whether feeding improves after the release. A fast procedure only helps if it leads to better function.
What to ask before deciding on treatment

Before choosing treatment, ask how the tie is affecting your baby’s actual feeding. The label matters less than the full picture, so look at latch, weight gain, pain, and how feeds are going day to day.
A few good questions can guide the conversation:
- Are feeding problems really tied to tongue movement?
- What are the benefits of trying more lactation support first?
- What risks or downsides come with frenotomy?
- Who should do the procedure, and how often do they perform it?
- How will we know if treatment worked?
You can also ask whether the person recommending treatment has watched a feeding. That matters because the diagnosis label alone should not drive the decision. A baby with a visible tie and normal feeding may not need anything beyond follow-up.
If symptoms are mild, watchful waiting plus support may be enough. If pain, poor latch, or slow weight gain continue, then frenotomy becomes a more practical option. The best choice is the one that matches your baby’s feeding needs, not just the exam result.
Myths, facts, and when to get help
Tongue-tie gets talked about a lot, and that can make it harder to sort facts from fear. Some babies truly need treatment, while others just need watchful follow-up and better feeding support.
The key is simple, function matters more than appearance. A visible tie alone does not tell you whether it is a problem. What matters is how your baby feeds, grows, and feels during and after feeds.
Common tongue-tie myths parents hear
One common myth is that all tongue-ties need surgery. They don’t. Many babies with a tight frenulum feed well and never need a procedure, especially if latch and positioning are good.
Another myth is that a heart-shaped tongue always means a severe problem. That shape can be a clue, but it does not measure how well the tongue works. Some babies with a heart-shaped tongue feed fine, while others with a less obvious tie struggle.
A third myth is that tongue-tie always causes speech delays. That’s not true either. Some children never develop speech issues, and many speech problems come from other causes. For a plain overview of how tongue-tie affects infants, Cleveland Clinic’s tongue-tie guide explains the condition well.
A tongue-tie diagnosis is only part of the picture. The real question is whether it affects feeding or later oral function.
In short, don’t let the shape of the tongue decide everything. Watch the feeding, the comfort, and the weight gain.
When to seek a professional evaluation
Get your baby checked if feeds are painful for you, even after trying better latch support. Ongoing nipple pain, cracking, or pinching is a strong reason to ask for help.
Also call a doctor or lactation consultant if you notice:
- poor weight gain
- low diaper output
- feeds that take too long
- trouble staying latched
- clicking, popping off, or weak suction
- baby seeming tired or unsatisfied after feeds

A baby who isn’t transferring milk well may need prompt support, especially in the first weeks. The HealthyChildren tongue-tie guide also notes that feeding problems deserve attention, not guesswork.
If you’re unsure, trust the pattern. Painful feeds, poor growth, and weak milk transfer are the red flags that should not wait.
Conclusion
Tongue-tie is a restriction in tongue movement, not just a certain look under the tongue. Many babies feed well with a mild tie, but some need feeding support or treatment when latch, milk transfer, or comfort starts to suffer.
The main takeaway is to watch function. If feeds are painful, slow, or not effective, early evaluation can point you in the right direction and keep problems from piling up.
With the right help, parents can feel more confident, and babies can feed more comfortably.
Save the pin for later

- 12 Things Pregnant Women Do When They’re Alone - June 7, 2026
- 25 Healthy Pregnancy Snacks You Should Try - June 7, 2026
- 100 Funny Baby Jokes That Will Make You Laugh - May 15, 2026

