
Malaria During Pregnancy is more dangerous than malaria in many other adults because pregnancy lowers your immune defenses, and the parasites can collect in the placenta. That can reduce oxygen and nutrients to your baby, while also raising your risk of severe illness. Recent CDC guidance also notes that pregnant women are about 3 times more likely to develop severe malaria.
Because of that, symptoms like fever, chills, headache, vomiting, and body aches should never be brushed off during pregnancy, especially after travel or time in a malaria area. This post will walk you through the risks, common symptoms, warning signs, diagnosis, treatment, prevention, and when to get urgent care, along with a few practical pregnancy safety reminders, including foods toxic to your unborn baby. Start with the signs that need quick medical attention, because early care can protect both you and your baby.
How malaria affects the body during pregnancy
Malaria During Pregnancy can hit harder and cause more damage than many people expect. The infection does not just cause fever and chills. It can strain the mother’s blood supply, lower oxygen delivery, and interfere with how the placenta supports the baby.
That is why quick testing and treatment matter so much. According to the CDC guidance for pregnant women and malaria care, pregnancy raises the risk of severe disease, which means symptoms should never be brushed off after travel or exposure in a malaria area.
Why pregnancy makes malaria more dangerous
During pregnancy, the immune system shifts so the body can support the baby. That change is normal, but it also makes it easier for malaria parasites to gain ground. As a result, a pregnant woman may get sicker faster than a non-pregnant adult exposed to the same infection.
Malaria also attacks red blood cells. When those cells drop, anemia can follow. That matters even more in pregnancy because the body already needs extra blood and extra oxygen for the baby. If malaria cuts into that supply, the mother can feel weak, dizzy, short of breath, or worn down much faster.

Another problem is that pregnancy can blur the early warning signs. A fever, body aches, nausea, or fatigue may sound like a virus or even normal pregnancy discomfort. Because of that, malaria can be missed at first, and a delayed diagnosis gives the infection more time to spread.
Severe malaria can affect the whole body, not just one system. It may lead to:
- High fever and dehydration, which can make a pregnant woman feel wiped out very quickly
- Severe anemia, which lowers oxygen delivery to both mother and baby
- Low blood sugar, especially in very sick patients
- Breathing problems or organ stress, which need urgent hospital care
A recent systematic review on malaria in pregnancy also points to the same pattern: pregnant women face higher risks of severe illness, anemia, poor birth outcomes, and complications linked to the placenta. In plain terms, pregnancy gives malaria more chances to do harm, and less time should be wasted before treatment starts.
In pregnancy, malaria is not “just a fever.” It can become a fast-moving illness that affects both mother and baby at the same time.
What placental malaria means for the baby
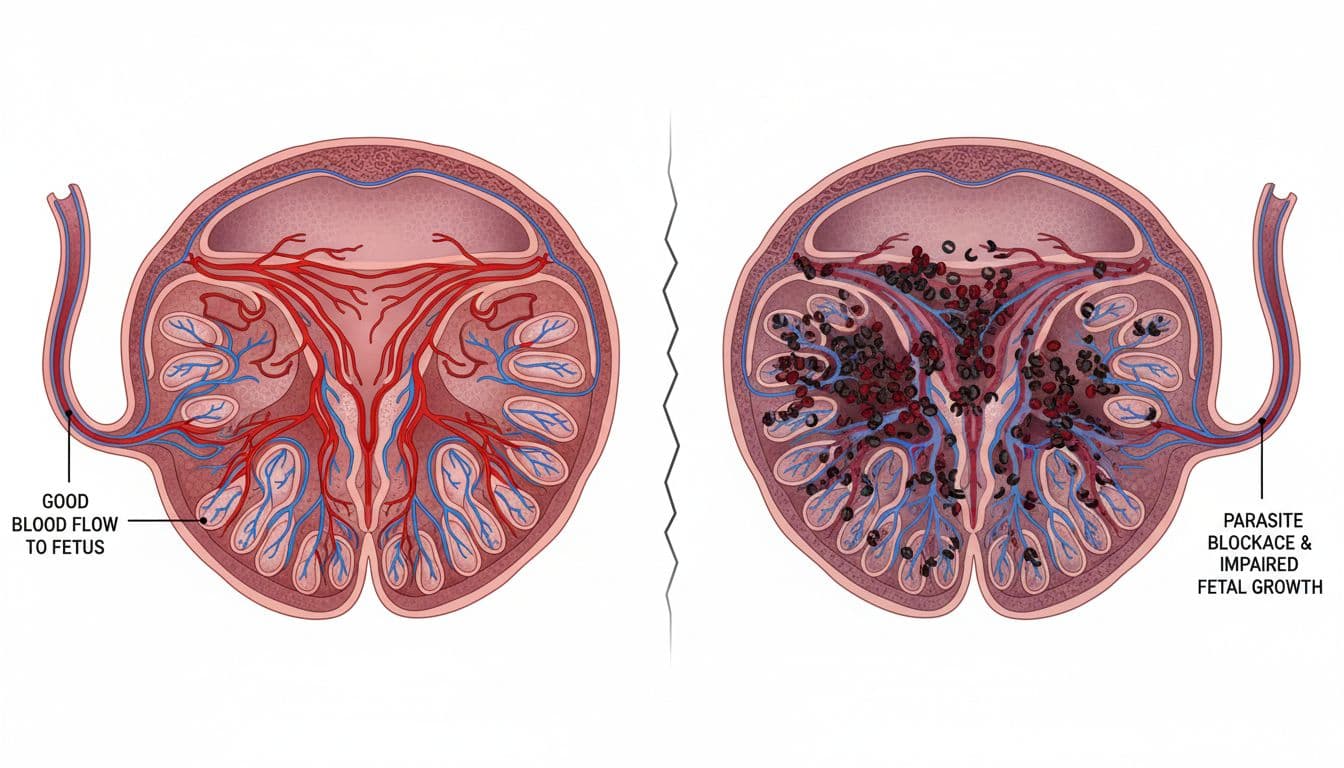
One of the biggest dangers in Malaria During Pregnancy is placental malaria. This happens when infected blood cells collect in the placenta instead of moving through normally. The placenta is the baby’s lifeline, so any blockage there can create trouble.
When the placenta is inflamed or clogged with infected cells, it may not pass enough oxygen and nutrients to the baby. The baby may still be growing, but growth can slow down over time. In simple terms, the baby is getting less of what it needs, like a garden hose with a kink in it.
This can lead to a few major problems. The most common ones include:
- Poor growth in the womb, which means the baby may be smaller than expected
- Low birth weight, even if the baby is born close to the due date
- Preterm birth, when labor starts too early
- Higher risk of stillbirth or newborn illness in severe cases
Low birth weight is especially important because it can affect how well a newborn handles the first days and weeks of life. Smaller babies may have a harder time staying warm, feeding well, and fighting infection. So even when the baby survives the pregnancy, placental malaria can still create a rough start.
The timing matters too. If malaria affects the placenta early or keeps coming back, the baby may have less time and less support for steady growth. If it triggers early labor, the baby may be born before the lungs and other systems are fully ready.
First pregnancies often carry more risk because the body has less built-up protection against the way malaria parasites attach in the placenta. That helps explain why some pregnant women become very sick, while others still have infection but fewer obvious signs. Either way, the placenta can be affected, which is why early testing is so important after fever or travel exposure.
The biggest risks for mom and baby
Malaria During Pregnancy can move from “feeling sick” to a medical emergency much faster than many people realize. The infection can harm the mother directly, and at the same time reduce the placenta’s ability to support the baby. Because of that, the biggest risks are not limited to fever alone. They include serious blood, organ, pregnancy, and birth problems that need quick care.
Health risks for the mother
For the mother, malaria often starts with fever, chills, weakness, vomiting, and body aches, but it can worsen quickly. Fever can drive dehydration, especially if you’re already vomiting or not able to drink enough. In pregnancy, that can leave you drained fast and make dizziness, faintness, and a racing heart more likely.
Malaria also destroys red blood cells, so anemia is common. That matters even more in pregnancy because your body already needs extra oxygen and blood flow. If anemia becomes severe, you may feel short of breath, exhausted, pale, or too weak to function normally.

Another danger is low blood sugar, which can happen with malaria itself and may be harder to spot during pregnancy. That can cause shaking, sweating, confusion, or sudden weakness. According to CDC guidance for pregnant women with malaria, pregnant women face a higher risk of severe disease, so symptoms should never be brushed aside after travel or exposure.
If the infection becomes severe malaria, it can affect the lungs, kidneys, liver, or brain. Some women develop breathing trouble, kidney injury, seizures, or other organ complications that need hospital treatment right away. In rare cases, death can happen if malaria is not treated quickly, which is why early testing matters so much.
Pregnancy and birth risks for the baby
When malaria affects pregnancy, the baby may suffer even before labor begins. The infection can inflame the placenta and reduce the baby’s access to oxygen and nutrients. Over time, that can slow growth and raise the chance of poor fetal growth and low birth weight.
The risks can also start earlier in pregnancy. Malaria During Pregnancy is linked to miscarriage, especially when infection is severe or treatment is delayed. That risk adds to other early pregnancy concerns, including foods that cause miscarriage in early pregnancy, which is why any illness during pregnancy deserves prompt attention.
Labor and delivery can be affected too. Malaria raises the chance of preterm birth, which means a baby may arrive before the lungs and other organs are fully ready. It also increases the risk of stillbirth in serious cases. The WHO notes that malaria in pregnancy remains a major cause of poor outcomes for mothers and babies in high-burden areas, including stillbirth and newborn death.

After birth, some newborns may also face infection related to malaria exposure, sometimes called congenital or newborn malaria. This is not the most common outcome, but it can happen. A baby with infection may have fever, poor feeding, sleepiness, or low energy, so pediatric follow-up matters if malaria occurred during pregnancy.
The baby’s risk does not begin at delivery. It often starts when malaria disrupts the placenta weeks earlier.
Who may face the highest risk
Some pregnant women face a steeper climb than others. Risk is often higher in a first pregnancy, because the body has less built-up protection against the way malaria parasites stick to the placenta. That is one reason first-time moms can get sicker, even when symptoms seem mild at first.
Risk also rises when a woman has limited immunity, including travelers from the US who do not live in malaria-endemic regions. If you travel to a place where malaria is common, your body may have little natural defense. The CDC advises pregnant travelers to avoid malaria areas when possible because no prevention plan works perfectly, as explained in its pregnant traveler malaria advice.
Delayed testing is another major problem. Malaria can look like flu, a stomach bug, or routine pregnancy sickness in the early stage. If testing is put off, the infection has more time to spread. Lack of prenatal care adds another layer of risk because warning signs, anemia, and fetal growth problems may be missed until the illness is more advanced.
Symptoms to watch for, and signs that mean get help now
Malaria During Pregnancy can start with symptoms that look a lot like flu, a stomach bug, or even rough pregnancy days. That overlap is why it gets missed. If you’ve had possible exposure, even “ordinary” symptoms deserve quick attention, because malaria can worsen fast in pregnancy.
Common malaria symptoms in pregnancy
The early signs often sound familiar, which is part of the problem. You may notice fever, chills, sweating, a headache, body aches, nausea, vomiting, and strong fatigue. Some women also feel generally weak, shaky, or too drained to do normal tasks.

Because pregnancy already causes tiredness and nausea, it’s easy to second-guess what you’re feeling. Still, malaria tends to make you feel more suddenly sick, more feverish, and more wiped out than usual. According to the CDC’s overview of malaria symptoms, symptoms can range from mild to severe, and they should be taken seriously after travel or mosquito exposure.
Some pregnant women also develop anemia, which can lead to dizziness, shortness of breath, paleness, and a heavy feeling of exhaustion. If you’re already run down, symptoms tied to preventing anemia symptoms like fatigue can stack on top of malaria and make daily life feel much harder.
A simple rule helps here: if you are pregnant, have fever or flu-like illness, and there is any malaria risk, get tested quickly. Waiting to “see if it passes” can cost valuable time.
Emergency warning signs that should never wait
Some symptoms mean the illness may be turning severe, and that needs urgent care right away. Get emergency help if you have trouble breathing, confusion, severe weakness, fainting, seizures, yellow skin or eyes, a very high fever, clear signs of dehydration, reduced fetal movement, or you can’t keep fluids down.

Dehydration can show up as a very dry mouth, little or no urine, dizziness when standing, or a racing heart. Reduced fetal movement matters too. If your baby is moving less than usual while you’re sick, don’t wait for the next day.
The WHO malaria fact sheet and WHO guidance on severe symptoms both warn that breathing problems, seizures, jaundice, and impaired alertness can signal severe malaria. In pregnancy, those red flags matter even more because both mother and baby can decline quickly.
If symptoms feel intense, fast-moving, or “not right,” treat that as urgent and get medical help now.
If you’re in the US and recently traveled, tell the clinic or ER about that right away. Malaria is treatable, but speed matters.
How doctors confirm malaria and choose safe treatment
With Malaria During Pregnancy, doctors do not rely on symptoms alone. Fever, chills, vomiting, and body aches can overlap with many other illnesses, so the goal is to confirm the infection fast and then match treatment to the exact type of malaria. That helps protect both you and the baby, and it lowers the risk of delays or the wrong medicine.
Tests used to diagnose malaria
The first clue is often your travel and exposure history. A doctor will want to know where you’ve been, when you traveled, whether you had mosquito bites, and when symptoms started. In the US, that travel history matters a lot, because malaria is uncommon here and can be missed if no one asks.
Doctors then confirm malaria with a blood test, not by symptoms alone. According to the CDC’s malaria testing guidance, the main test is a blood smear, where a lab looks at your blood under a microscope for parasites. Some clinics also use rapid tests, but microscopy is still important because it can show how much parasite is in the blood and which species is present, as explained in WHO guidance on malaria microscopy.

Identifying the parasite matters because malaria is not one-size-fits-all. Different species can act differently, and some are more likely to resist certain drugs. Your clinician also looks at how severe the infection is, because a mild case and a dangerous case do not get treated the same way.
Safe care for uncomplicated malaria during pregnancy
If malaria is confirmed and it is not severe, treatment still needs careful planning. A qualified clinician must choose the treatment, because pregnancy changes what is safest and what works best. That choice depends on the parasite species, where the infection was picked up, local drug resistance, and your trimester.
The good news is that pregnancy-safe antimalarial medicines are available. Current CDC guidance for pregnant women with malaria makes clear that doctors can treat uncomplicated malaria in pregnancy with medicines chosen for both safety and effectiveness. Your doctor may also order repeat blood tests after treatment starts, because they need to confirm the parasites are clearing.
This is why self-treating is risky. A medicine that is right for one traveler may be wrong in pregnancy, or wrong for the species causing your infection. In simple terms, doctors are matching the drug to the parasite, the place of exposure, and the stage of pregnancy, all at once.
Safe treatment exists, but it has to be the right treatment for your pregnancy and your infection.
What happens if malaria becomes severe
Severe malaria is a medical emergency. It can affect the brain, lungs, kidneys, blood sugar, and blood counts in a short time. In pregnancy, doctors usually admit patients to the hospital right away because both mother and baby may need close observation.
Hospital care often includes IV antimalarial treatment, frequent vital sign checks, blood work, and support for problems such as low blood sugar, anemia, or dehydration. The CDC’s severe malaria treatment guidance stresses that severe cases need prompt treatment because the illness can worsen quickly.

Doctors may also give fluids carefully and watch for breathing trouble or other organ stress. When appropriate, they check on the baby with fetal monitoring or other pregnancy-specific assessments. The main goal is simple: stabilize the mother fast, clear the parasite, and keep a close eye on the baby’s well-being while treatment is underway.
Prevention steps that can lower the risk
Preventing Malaria During Pregnancy starts with one simple goal, keep mosquito bites from happening and catch problems early if exposure is possible. No single step gives perfect protection, so the safest plan layers daily habits, travel advice, and regular prenatal care. That matters even more in pregnancy, because even a short delay can raise the risk for both you and your baby.
How to avoid mosquito bites day and night
The best everyday protection is to make it hard for mosquitoes to reach you. At night, sleep under an insecticide-treated bed net every time, not just when bugs seem bad. These nets do two jobs at once, they create a barrier and also kill or repel mosquitoes that land on them. The WHO continues to recommend insecticide-treated nets in pregnancy because they lower malaria risk for both mother and baby.

During the day and evening, clothing helps more than many people expect. Wear long sleeves, long pants, socks, and loose-fitting layers when possible, especially around dusk and dawn. Mosquitoes do not care that you are indoors either, so keep window screens and door screens in good repair, and use air conditioning when available.
Repellent also matters. In plain terms, a pregnancy-safe repellent gives your skin an extra shield. The key is to use it the right way:
- Apply repellent to exposed skin and, if needed, to clothing as directed on the label.
- Follow the product label carefully, because more is not better.
- Avoid putting repellent on cuts, irritated skin, or near your eyes and mouth.
- Wash it off when you come indoors for the day, if the label recommends that.
If you live in or travel through a malaria area, combining a bed net, covered clothing, screens, and repellent is much stronger than relying on only one step. It is a lot like locking your front door and your windows, not just one of them.
Bed nets, clothing, screens, and repellent work best as a package, not as separate backup plans.
What to know before travel to a malaria-risk area
If you are pregnant and planning international travel, get medical advice before the trip, not after you arrive. Some destinations carry a very high malaria risk, and for pregnant travelers from the US, the CDC advises avoiding malaria areas when possible because pregnancy raises the chance of severe illness. The current CDC guidance for pregnant women and malaria makes that point very clear.

Pre-travel care matters because malaria prevention medicine in pregnancy must be chosen with care. The right option depends on where you are going, which malaria species are common there, and whether drug resistance is known in that area. A medicine that works in one country may be the wrong pick in another.
Before travel, ask your clinician or travel medicine provider about:
- Whether the trip should be postponed or changed.
- Which prevention medicine is considered safest for your stage of pregnancy.
- When to start the medicine, because some options begin before departure.
- What to do if you develop fever during the trip or after you return.
This step is not something to handle with online guesswork. Even short trips can carry risk, and symptoms may not start right away. If you must travel, use prevention medicine exactly as prescribed and keep up all bite-avoidance steps the whole time.
Why prenatal visits matter in malaria-prone areas
In malaria-prone areas, prenatal visits are more than routine check-ins. They give your care team chances to look for early warning signs, track anemia, watch your baby’s growth, and offer prevention that fits local risk. If programs are available where you live, your clinic may also provide community-based malaria prevention or pregnancy-specific malaria services.
WHO guidance also supports intermittent preventive treatment in pregnancy in certain malaria-endemic settings. In those areas, eligible pregnant patients may receive preventive doses during prenatal care, starting in the second trimester, under local guidelines. You can read more in the WHO page on preventive treatment to reduce malaria risk during pregnancy.
Just as important, prenatal visits give you a place to report symptoms early. Tell your clinician right away about fever, chills, vomiting, unusual weakness, dizziness, or reduced fetal movement, especially if you live in, or recently traveled to, a malaria area. Early testing can prevent a small problem from turning into a hospital-level emergency.
If you were treated for malaria during pregnancy, follow-up matters too. Your doctor may want repeat blood tests, anemia checks, or extra monitoring for the baby. That follow-up helps confirm the infection cleared and that both you and your baby are recovering well.
Conclusion
Malaria During Pregnancy is a serious illness, not something to watch and wait on. Because it can harm the mother, the placenta, and the baby at the same time, early care makes a real difference.
The biggest takeaway is simple, don’t ignore fever, chills, vomiting, weakness, or flu-like symptoms if there’s any chance of malaria exposure. Prompt testing and the right treatment can protect your health, support your baby’s growth, and lower the risk of severe complications.
Prevention matters too, especially during travel or in malaria-prone areas. If you’re pregnant and think you may have malaria, or you’ve had a fever after possible exposure, contact your doctor, midwife, or urgent care right away.
Save the pin for later

- 12 Things Pregnant Women Do When They’re Alone - June 7, 2026
- 25 Healthy Pregnancy Snacks You Should Try - June 7, 2026
- 100 Funny Baby Jokes That Will Make You Laugh - May 15, 2026

